RA and Microscopic Polyangiitis: Overlap Syndrome or Vasculitis Subset?
A 54-year-old Asian woman presented with ongoing renal insufficiency and anemia that were thought to be the result of analgesic nephropathy caused by NSAIDs.
ABSTRACT:The woman presented with ongoing renal insufficiency and anemia. She had received a diagnosis of bilateral scleritis 8 years earlier. More recently, she experienced elbow pain, swelling, and decreased range of motion. A review of symptoms was negative for eye pain and visual complaints, photophobia, rash, oral ulcers, and Raynaud phenomenon. Physical examination findings were mostly normal. Laboratory findings were significant for a positive rheumatoid factor. Elbow MRI scans showed generalized synovitis and marked synovial proliferation. A renal biopsy specimen revealed a pauci-immune glomerulonephritis with crescents. The diagnosis of bilateral scleritis could be attributed to a subsequent diagnosis of rheumatoid arthritis or to a new diagnosis of antineutrophil cytoplasmic autoantibody vasculitis. The case demonstrates how a common rheumatologic condition may present in an uncommon way.
A 54-year-old Asian woman presented with ongoing renal insufficiency and anemia that were thought to be the result of analgesic nephropathy caused by NSAIDs. Her medical history also was significant for hypertension that was well controlled. In this article, we describe her case to demonstrate how a common rheumatologic condition may present in an uncommon way.
Case Presentation
Eight years earlier, the patient received a diagnosis of bilateral scleritis and also had mild joint discomfort. She was treated with methotrexate and corticosteroids; there was good resolution of her symptoms.
Over the past year, the patient experienced right elbow pain and swelling, followed by decreased range of motion. A review of symptoms was negative for eye pain and visual complaints, photophobia, rash, oral ulcers, and Raynaud phenomenon. She had no other joint complaints and no morning stiffness. There was no history of blood clots, epistaxis, or hemoptysis.
Findings from the patient's physical examination were normal except for a blood pressure of 199/70 mm Hg (normal, 120/80 mm Hg) and a painful, swollen right elbow with decreased extension. Her hand, wrist, shoulder, knee, ankle, and foot joints did not show synovitis and were not tender. Her sclera were not injected, and the results of an eye examination were otherwise unremarkable.
Laboratory findings were significant for a positive rheumatoid factor (RF) at 40.2 IU/mL (normal, lower than 13 IU/mL) and an anti–cyclic citrullinated peptide (anti-CCP) antibody level of 24 U/mL (normal, lower than 7 U/mL), perinuclear antineutrophil cytoplasmic antibodies (pANCA) titer of 1:320 (normal, lower than 1:20), and myeloperoxidase (MPO) antibody level of 40.2 IU/mL (normal, lower than 9 IU/mL). Her antinuclear antibody test result was negative, and C3 and C4 levels were normal. Her erythrocyte sedimentation rate was 68 mm/h (normal, 0 to 20 mm/h), and her creatinine and hemoglobin levels were 1.46 mg/dL (normal, 0.7 to 1.2 mg/dL) and 7.1 g/dL (normal, 13.5 to 18 g/dL), respectively; urinalysis did not show an active sediment.
FIGURE 1


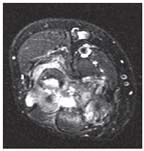
A coronal view of the patient's right elbow shows erosions and synovial thickening.
MRI scans of the patient's right elbow obtained without contrast showed generalized synovitis and marked synovial proliferation along with a joint effusion (Figures 1 and 2). There also was extensive erosive arthropathy. A renal biopsy specimen revealed a pauci-immune glomerulonephritis with crescents (Figure 3).
Given the biopsy results, the patient received 500 mg of methylprednisolone intravenously for 3 days and then therapy was transitioned to prednisone, 60 mg/d. Therapy with cyclophosphamide, 100 mg PO daily, also was started. In addition, the patient received atovaquone for Pneumocystis jiroveci pneumonia prophylaxis because she had a sulfa allergy. Calcium plus vitamin D and nasal calcitonin were given concomitantly with her prednisone for bone health protection.
FIGURE 2



A sagittal view of the patient's elbow shows chondromalacia and synovial thickening.
Discussion
The diagnosis of bilateral scleritis that the patient received 8 years earlier could be attributed to a subsequent diagnosis of rheumatoid arthritis (RA) or to a new diagnosis of antineutrophil cytoplasmic autoantibody (ANCA) vasculitis. The physical examination and MRI findings for her elbow, in addition to her positive anti-CCP antibody test result, strongly suggest that she has RA, but the renal biopsy specimen indicates a renal vasculitis. Because having these two diseases at the same time is very unusual, the question becomes, Is the patient's condition an overlap syndrome of two diseases that do not occur together frequently or a subset of rheumatoid vasculitis?
FIGURE 3


The patient's renal biopsy specimen revealed a pauci-immune glomerulonephritis with crescents.
Rheumatoid vasculitis usually occurs in patients who are RF-positive and have long-standing disease that has gone untreated. The most common findings are nail bed infarctions (not present in our patient) and mononeuritis multiplex (which our patient also did not have) found by history or examination.
Patients with RA have been reported to have positive pANCA titers, but having a concurrent ANCA vasculitis is quite rare. There have been reports of RA overlapping with granulomatosis with polyangiitis (formerly Wegener granulomatosis), microscopic polyangiitis, and Churg-Strauss syndrome.1
Our patient probably has RA–microscopic polyangiitis overlap syndrome. Treatment should be chosen to manage both conditions. The agents most frequently used are corticosteroids and other disease-modifying antirheumatic drugs, such as methotrexate and azathioprine. Rituximab often is used for severe RA and recently was approved for treatment of patients with ANCA vasculitides.2 One case series, currently in abstract form, recently suggested that the use of rituximab was beneficial in 3 cases of these overlap syndromes.1
Our patient initially will receive oral cyclophosphamide for 6 to 9 months, with a likely change to azathioprine or methotrexate for maintenance therapy. If she relapses or if therapy with cylcophosphamide is not successful, rituximab will be a likely option; it could have been the initial choice for therapy.
The patient's prednisone regimen currently is reduced to 15 mg/d. At her last visit, she received an intra-articular corticosteroid injection into the right elbow. With regard to her renal function, her overlap syndrome is responding nicely to treatment-her most recent creatinine level was 1.08 mg/dL. Repeated MPO and pANCA testing are pending.
References:
REFERENCES
1. Szilasi M, Mátyus J, File I, et al. Association of ANCA-associated vasculitis-rheumatoid arthritis overlap syndrome in four patients: rituximab may be the right choice? Autoimmunity. 2012;45:304-309.
2. Stone JH, Merkel PA, Spiera R, et al; RAVE-ITN Research Group. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med. 2010;363:221-232.














