RA and Carotid Plaques: Five Things to Know
Patients with rheumatoid arthritis are at considerably increased risk of asymptomatic carotid artery disease, but standard scores have proven poor predictors of their actual cardiovascular risk. Special vigilance is warranted for these patients.
1. Patients with rheumatoid arthritis (RA) have twice as many atherosclerotic plaques in their carotid arteries as do people unaffected by RA. A study involving 152 RA patients and 89 controls has shown that plaques were more numerous in RA patients and also more likely to be present bilaterally.1,2 A comparative sonography study localized these plaques, showing specifically that intima media thickness in the proximal internal carotid artery is significantly greater among RA patients than among controls.3


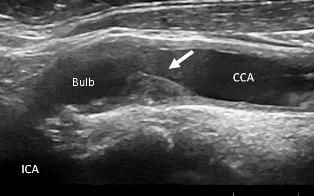
Arrow: Asymptomatic, vulnerable carotid artery plaque in a patient
with rheumatoid arthritis. CCA: common carotid artery, Bulb: bulbus
of carotid artery, ICA: internal carotid artery
2. Standard cardiovascular risk scores are poor predictors of asymptomatic carotid plaques in RA. Markers of preclinical atherosclerosis in RA patients are similar to those in people who have diabetes, suggesting that cardiovascular risk should be addressed as aggressively in RA as in diabetes.4 However, standard cardiovascular risk scores as European heart SCORE, Framingham and Reynolds CV risk algorithms, are poor predictors of asymptomatic carotid plaque (a-CP) in patients with inflammatory joint disease. Optimizing the cut off by closest point (0, 1) or 80% specificity did not improve identification of a-CP. 5
3. There is a high risk of classifying RA patients to a less intensive lipid-lowering regimen than that recommended by current guidelines. In a study of patients with rheumatoid arthritis (n=210), ankylosing spondylitis (n=87) and psoriatic arthritis (n=49), one third of those identified by the EAS/ESC SCORE cardiovascular risk scale as low risk (<5%) and therefore in no need of lipid-lowering therapy, or one in five similarly classed as low risk (<10%) according to the Framingham measures, had ultrasound evidence of carotid plaques. Carotid ultrasound contributes to correct classification of patients with inflammatory joint disease who require intensive lipid-lowering therapy for about 1/3 of patients with SCORE<5% and 2/3 of patients with SCORE>5%, with the same trends for Framingham and Reynolds.5
4. The risk of asymptomatic carotid plaques provides yet another good reason to strive for early and sustained remission in RA. Autopsy studies of coronary artery plaques suggested that those in RA patients were more inflammatory and unstable, and less atherosclerotic, than those among controls who did not have RA.6 Similarly, patients with active RA as assessed by the Clinical Disease Activity Index have carotid plaques more vulnerable to rupture than do patients in remission, judging from the ultrasound characteristics of the plaques.1
5. Would prophylactic treatment with statins reduce the risk of plaque-related events in RA? There is little evidence concerning the effect of statins on the morphology of carotid plaques in patients with RA. However, our group at Diakonhjemmet Hospital in Oslo is conducting a trial on the effect of statins on carotid plaques (RORA-AS 1 study), and results are expected later this year.7
References:
REFERENCES:
1. Semb AG, Rollefstad S, Provan SA et al.Carotid Plaque Characteristics and Disease Activity in Rheumatoid Arthritis.J Rheumatol (2013) 40:4-10.
2. Roman MJ, Moeller E, Davis A, et al,Preclinical carotid atherosclerosis in patients with rheumatoid arthritis.Ann. Intern. Med. (2006) 144:249-256
3. Kobayashi H, Giles JT, Polak JF et al.Increased Prevalence of Carotid Artery Atherosclerosis in Rheumatoid Arthritis Is Artery-specific.J Rheumatol (2010) 37:3
4. Stamatelopoulos KS, Kitas GD, Papamichael CM et al.Atherosclerosis in Rheumatoid Arthritis Versus Diabetes: A Comparative Study. Arterioscler Thromb Vasc Biol (2009) 29:1702-1708
5. Semb AG, Rollefstad S, Olsen IC et al.The Presence of Asymptomatic Carotid Plaques in Patients with Inflammatory Joint Disease Results in Inadequate Treatment to Lipid Targets in Cardiovascular Disease Prevention. Abstract #69 (2012) American College of Rheumatology Annual Meeting.
6. Aubry M-C, Maradit-Kremers H, Reinalda MS et al.Differences in Atherosclerotic Coronary Heart Disease Between Subjects with and without Rheumatoid ArthritisJ Rheumatol 2007;34:937–42
7. Effects of Rosuvastatin on Carotid Artery Plaques in Patients With Inflammatory Joint Disease














